Carpal Tunnel Syndrome
Median nerve compression at the wrist
Overview
The Science of Carpal Tunnel Syndrome
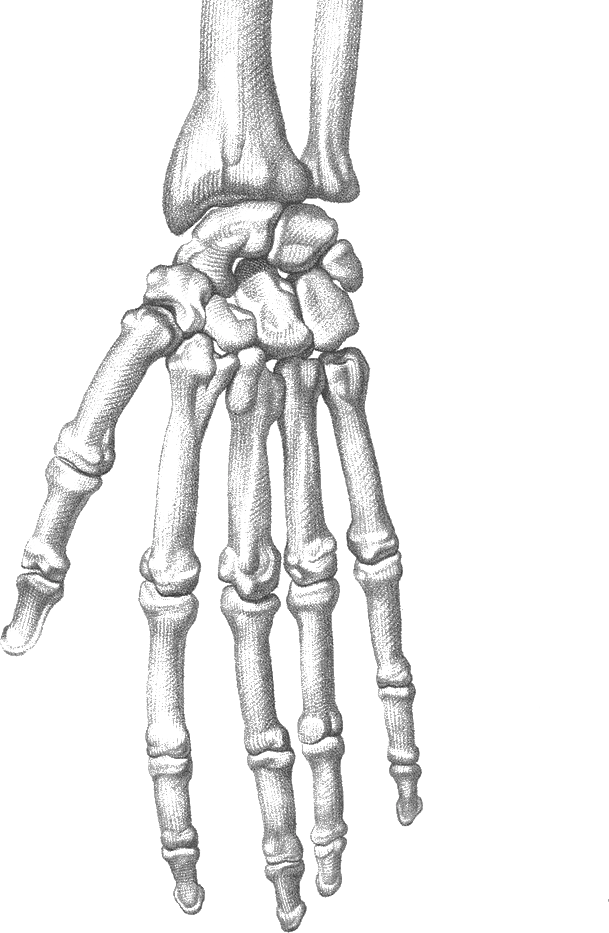
Link copiedsyndrome (CTS) is a peripheral nerve compression resulting from increased pressure on the as it passes through the carpal tunnel at the wrist. The carpal tunnel is an anatomically confined space bounded by carpal bones dorsally and the transverse carpal ligament (flexor ) volarly. Nine flexor tendons (four flexor digitorum superficialis, four flexor digitorum profundus, and flexor pollicis longus) pass through this tunnel alongside the median nerve, creating potential for compression when tunnel pressure exceeds capillary perfusion pressure (30 mmHg).
The pathophysiological cascade begins with mechanical compression causing impaired microvascular blood flow to the nerve (ischemia) and reduced venous drainage (congestion). This leads to nerve edema, further increasing tunnel pressure in a vicious cycle. Initially, compression affects the myelin sheath causing focal demyelination at the compression site, manifesting as intermittent and nocturnal symptoms. With sustained compression, axonal develops, progressing from distal sensory fibers to motor fibers, eventually causing permanent sensory loss and muscle atrophy if untreated.
Multiple factors contribute to increased carpal tunnel pressure. (inflammation of the tendon sheaths) from repetitive motion increases the volume of contents within the fixed-space tunnel. Systemic conditions including pregnancy (fluid retention), hypothyroidism (myxedematous tissue accumulation), rheumatoid (synovial inflammation), diabetes mellitus (metabolic factors affecting nerves), and obesity (increased tissue pressure) predispose to CTS. Anatomical variations such as persistent median artery, aberrant muscles within the tunnel, or smaller tunnel dimensions increase baseline pressure. Wrist position dramatically affects tunnel pressure - wrist flexion increases pressure to 90 mmHg while extension increases it to 110 mmHg compared to 32 mmHg in neutral position.
The median nerve provides sensory innervation to the palmar aspect of the thumb, index, middle, and radial half of the ring finger, plus motor innervation to the thenar muscles (abductor pollicis brevis, opponens pollicis, superficial head of flexor pollicis brevis) responsible for thumb opposition and . This explains the characteristic sensory distribution and eventual thumb weakness in advanced CTS. The condition often coexists with , , or pronator syndrome (double or triple crush phenomenon), where proximal nerve compression makes distal compression sites more symptomatic.
Risk factors include female gender (3:1 ratio, likely due to smaller tunnel anatomy and hormonal influences), age 40-60 years (peak incidence), pregnancy (third trimester fluid retention), obesity (BMI greater than 29), diabetes mellitus (2-3 times higher prevalence), hypothyroidism, rheumatoid arthritis, wrist trauma or fracture history, and occupations requiring repetitive forceful gripping, sustained wrist flexion/extension, or vibration exposure (assembly line work, meat processing, construction, computer-intensive work).
Overview
Contributing Factors
Link copiedThe biomechanical drivers of syndrome center on sustained or repetitive wrist postures and hand activities that increase intracarpal tunnel pressure. Wrist position has the most dramatic effect - neutral position maintains tunnel pressure around 30-32 mmHg, while wrist flexion increases pressure to 90 mmHg and wrist extension to 110 mmHg. Combined flexion or extension with finger flexion (gripping) can elevate pressure to 150-200 mmHg, exceeding capillary perfusion pressure and causing nerve ischemia.
Computer work represents a significant modern risk factor, though the mechanism is more complex than commonly assumed. During keyboard typing, the wrists typically rest in extension () if the keyboard is positioned too high relative to elbow height. Even mild extension of 15-20 degrees maintained for hours creates sustained elevated tunnel pressure. Mouse work is particularly problematic because it combines wrist extension with ulnar deviation and sustained static muscle contraction to control fine movements. The precision grip required for mouse control activates flexor tendons that further increase tunnel volume. Studies show computer users working more than 20 hours weekly have 2-4 times higher CTS incidence compared to non-computer workers.
Forceful gripping activities dramatically increase tunnel pressure through two mechanisms: increased flexor tendon excursion through the tunnel and increased muscle activation compressing the tunnel externally. Activities like using pliers, turning wrenches, carrying heavy bags by handles, or sustained power grip during manual labor can elevate tunnel pressure above 200 mmHg. Assembly line work requiring repeated forceful gripping with the wrist in non-neutral positions shows particularly high CTS rates. Vibration exposure from power tools compounds the problem by causing microtrauma to the nerve and promoting .
Repetitive finger movements, especially combined with wrist deviation, create cumulative trauma. During finger flexion and extension, the flexor tendons glide through the carpal tunnel - the more forceful and repetitive this movement, the greater the mechanical irritation and potential for tenosynovial thickening. Activities like playing musical instruments (piano, guitar, violin), assembly work, cashiering, or data entry that require thousands of repetitive finger movements daily create substantial cumulative mechanical stress. The combination of finger movement with wrist deviation (common in assembly tasks reaching to different stations) maximally increases tunnel pressure.
Sleeping postures significantly contribute to nocturnal symptoms - the hallmark of CTS. Most people sleep with wrists curled into flexion, either tucked under the pillow or pressed against the chest. This sustained flexion throughout 6-8 hours of sleep maintains elevated tunnel pressure, causing the characteristic awakening with hand numbness that requires shaking the hand to restore circulation. The supine sleeping position with wrists resting in flexion is particularly problematic. This explains why night splinting maintaining neutral wrist position effectively reduces nocturnal symptoms.
Sustained pinch grip activities create unique biomechanical stress. Fine manipulation tasks requiring sustained thumb-index finger pinch (sewing, knitting, crafts, detailed assembly work, using scissors) maintain continuous flexor tendon loading without relaxation periods. The sustained nature prevents recovery time between loading cycles, promoting inflammation. Smartphone and tablet use requiring sustained thumb reach and wrist flexion while supporting device weight contributes to modern CTS incidence.
Proximal factors influence distal nerve function through neural tension and vascular mechanisms. Forward head posture and rounded shoulders common in desk workers create increased neural tension throughout the and . This proximal tension makes the nerve more vulnerable to compression at the carpal tunnel (double crush phenomenon). compression can reduce nerve blood flow proximally, making the nerve more susceptible to ischemic damage from distal compression. Even dysfunction at C6-C7 (which contributes to median nerve formation) can create symptoms overlapping with or mimicking CTS.
Grip strength and hand size create biomechanical vulnerability. Individuals with smaller wrist circumferences have smaller carpal tunnels with less space for median nerve. Reduced grip strength forces people to grip harder to achieve the same task, increasing flexor tendon forces and tunnel pressure. Weak wrist stabilizers cause compensatory wrist movement during gripping tasks, forcing the wrist out of neutral position under load.
Symptoms
Clinical Presentation
Link copiedPrimary Symptoms
Associated Symptoms
Typical pattern
Gradual onset over weeks to months. Nocturnal symptoms most prominent early. Intermittent symptoms become progressively constant. Shaking hand relieves symptoms initially but becomes less effective over time. Symptoms often bilateral but may start unilateral or be asymmetric in severity.
Symptoms
Differential Diagnosis
Link copiedConditions with similar presentations:
Cervical Radiculopathy (C6 or C7)
Key differences: Neck-dominant pain that radiates into the arm in a pattern rather than distribution, positive Spurling's test, and weakness or sensory changes that follow a rather than sparing the small finger.
Pronator Syndrome (Median Nerve Compression in the Forearm)
Key differences: Aching along the volar proximal forearm, no clear nocturnal pattern, symptoms that often include the palmar cutaneous branch territory (central palm numbness, which is spared in classic syndrome), and reproduction of symptoms with resisted .
Thoracic Outlet Syndrome
Key differences: Symptoms across the whole hand rather than median distribution only, positional dependence (worse with arm elevation or carrying), associated neck and shoulder symptoms, and possible vascular features such as colour or temperature change.
Ulnar Nerve Entrapment at the Cubital Tunnel
Key differences: Numbness and tingling in the ring and small fingers (opposite distribution to ), worse with sustained elbow flexion, positive Tinel sign or elbow flexion test at the , and in advanced cases intrinsic hand weakness.
De Quervain's Tenosynovitis
Key differences: Sharp localised pain over the radial wrist at the first dorsal compartment, positive , no numbness or nocturnal pattern, and symptoms reproduced by thumb movement rather than by gripping or sustained wrist positions.
First Carpometacarpal Joint or Wrist Osteoarthritis
Key differences: Joint-line pain and morning stiffness, pain reproduced by joint loading rather than nerve provocation tests, visible joint changes on X-ray, and no characteristic nocturnal numbness pattern.
When to seek professional help
Research
Key Research & Evidence
Peer-reviewed studies supporting the treatment approach.
Finding
Night-time wrist splinting is associated with a higher rate of overall symptom improvement than no treatment in mild to moderate CTS
Research details
Cochrane systematic review (Karjalainen and colleagues, 2023) including 29 randomized trials with 1,937 adults found that wrist splinting may provide only small, uncertain benefits in symptoms and hand function compared with no active treatment (mean Boston Carpal Tunnel Questionnaire symptom score 0.37 points better, below the threshold considered clinically important; low-certainty evidence). The clearest signal was that night-time splinting was associated with a higher rate of overall improvement in the short term (risk ratio 3.86) than no treatment. As a low-cost intervention with no plausible long-term harm, splinting can be a reasonable first-line option, particularly for people not interested in injections or surgery
Clinical relevance
Night splinting represents first-line treatment with moderate effect sizes and sustained benefits for mild-moderate CTS. Neutral wrist position critical - extension splinting counterproductive. Patient education regarding consistent nightly use essential as compliance strongly predicts outcomes. Cost-effective intervention that prevents or delays surgery in majority of appropriate candidates
Finding
Corticosteroid injection superior to placebo at 4 weeks and 3 months but inferior to surgery at 12 months
Research details
Cochrane systematic review (Ashworth and colleagues, 2023) of 14 randomized trials with 994 participants found local corticosteroid injection probably improves symptoms compared with placebo at up to three months (standardized mean difference -0.77, 95% CI: -0.94 to -0.59) and at up to six months (SMD -0.58, 95% CI: -0.89 to -0.28), with a probable small reduction in the need for surgery at 12 months (risk ratio 0.84, 95% CI: 0.72 to 0.98); this was moderate-certainty evidence. A separate Cochrane review of surgical versus non-surgical treatment (Lusa, Karjalainen and colleagues, 2024; 14 trials, 1,231 participants) found surgery probably yields a higher rate of clinical improvement than splinting in the long term (risk ratio 2.10) but no clinically important difference in BCTQ symptom or function scores, while reducing later referral to surgery
Clinical relevance
Corticosteroid injection provides meaningful medium-term relief useful for patients preferring to avoid surgery, pregnant patients who cannot have surgery until postpartum, or as diagnostic trial before surgery. However, effect diminishes over 6-12 months with less than half maintaining benefit at one year. Not alternative to surgery for long-term management but valuable temporizing measure. Ultrasound guidance improves outcomes by ensuring accurate injection placement
Finding
More severe or persistent CTS tends to respond better to surgery than to continued conservative care
Research details
Cochrane systematic review of surgical versus non-surgical treatment for CTS (Lusa, Karjalainen and colleagues, 2024) pooled 14 randomized trials with 1,231 participants and found that surgery probably produces a higher rate of long-term clinical improvement than splinting (risk ratio 2.10, 95% CI: 1.04 to 4.24) and reduces later referral to surgery, though it does not provide a clinically important advantage in BCTQ symptom or function scores. The review notes that people with more severe symptoms, a strong preference for clinical improvement, and reluctance to persist with non-surgical options may reasonably choose surgery, while those with tolerable symptoms can start with non-surgical care and proceed to surgery only if needed
Clinical relevance
Severity stratification essential for treatment decisions. Mild-moderate cases warrant 8-12 week conservative trial with splinting and activity modification. Severe CTS with constant numbness, motor involvement, or symptoms over 12 months should proceed directly to surgical consultation as conservative treatment success rate too low to justify delayed definitive treatment that risks permanent nerve damage. Electrodiagnostic testing valuable for determining severity when clinical presentation unclear
Management
Evidence-Based Management
Treatment strategies with the strongest support in the current literature.
Primary approach
Night splinting in neutral wrist position reduces symptoms by 60-70% in mild to moderate cases over 4-12 weeks by preventing sustained wrist flexion during sleep that elevates pressure, with effects maintained long-term when combined with activity modification
Complementary
Nerve and tendon gliding exercises improve mobility through the and reduce adhesions, while corticosteroid injection provides short to medium-term symptom relief for moderate cases (3-6 months benefit) though effect diminishes over time
Prevention & long-term
Workplace ergonomic changes that maintain neutral wrist postures and regular micro-breaks reduce symptom severity in high-risk occupations, while grip strength training addresses modifiable risk factors
Detailed management strategies
Night Splinting in Neutral Wrist Position
Maintains wrist in neutral (straight) position during sleep, preventing sustained flexion that increases pressure to 90+ mmHg. Neutral position keeps pressure at baseline 30-32 mmHg, allowing nerve recovery. Reduces nocturnal symptoms in 60-70% of cases within 4 weeks
Important precautions
- Must wear consistently every night - intermittent use significantly less effective
- Ensure splint maintains neutral position, not extension (which also increases pressure)
- May feel awkward initially but most adapt within 1 week
- Continue for minimum 4-6 weeks even if symptoms improve quickly
Nerve and Tendon Gliding Exercises
Specific exercises that gently mobilize the and flexor tendons through the , reducing adhesions and improving nerve excursion. Increases nerve blood flow and reduces mechanical irritation. Perform 3-5 times daily
Important precautions
- Should not cause sharp pain or numbness - if so, reduce range or frequency
- Gentle controlled movements, not aggressive stretching
- Consistency more important than intensity
- Skip if symptoms severely aggravated, resume when tolerable
Ergonomic Workplace Modifications
Adjusting workstation setup to maintain neutral wrist postures during computer work and manual tasks. Keyboard at elbow height, mouse at same level, wrist rests used only during pauses (not while typing), neutral wrist pads for support. Reduces sustained loading in flexion or extension that elevates tunnel pressure
Important precautions
- Small changes in wrist angle create large changes in tunnel pressure - even 15 degrees matters
- Regular microbreaks (30 seconds every 20-30 minutes) to change position and perform nerve glides
- Consider vertical mouse to reduce forearm pronation
- Modify all repetitive activities, not just most obvious one
Activity Pacing and Task Modification
Identifying and temporarily reducing or modifying high-risk activities that require sustained wrist flexion/extension or forceful repetitive gripping. Allows nerve inflammation to settle while maintaining function through alternative movement strategies. Gradual progressive return to activities as symptoms improve
Important precautions
- Monitor symptom response 2-4 hours after activities and following morning
- Temporary symptom increase acceptable if resolves within 4 hours
- Avoid complete rest of hand - gentle movement within tolerance important
- Use adaptive equipment (jar openers, ergonomic tools) during symptom flare-ups
Addressing Systemic Contributing Factors
Identifying and managing underlying conditions that increase CTS risk including diabetes control, thyroid management, addressing pregnancy-related fluid retention, weight management if obese. These factors independently increase pressure and reduce nerve health
Important precautions
- Pregnancy-related CTS often resolves within weeks postpartum - consider symptom timeline before aggressive intervention
- Diabetes management important for nerve health beyond just CTS
- Even modest weight loss (5-10%) can reduce symptoms in obese patients
- Screen for other symptoms suggesting systemic conditions
Proximal Chain Assessment
Addressing neck posture, shoulder position, and mobility that influence nerve tension and blood flow from through the arm to wrist. Double crush phenomenon means proximal compression makes distal nerve more vulnerable. Improving proximal mechanics reduces neural tension
Important precautions
- Don't ignore neck and shoulder symptoms even though wrist is primary complaint
- Forward head posture and rounded shoulders increase neural tension throughout median nerve
- Thoracic outlet restrictions can contribute to symptoms
- Full nerve pathway from neck to hand should be assessed
Management
Treatment Techniques
Evidence-based manual therapy and intervention approaches.
Treatment approaches supported by current research and clinical guidelines
Recommended treatment approaches
Treatment approaches are individualized to each patient's needs and goals. All interventions require explicit informed consent, and treatment plans are collaboratively modified based on your preferences and response to care.
Dry Needling
Precise needle therapy targeting trigger points for effective pain relief and improved muscle function.
Soft Tissue & Myofascial Therapy
Targeted hands-on techniques to address muscle tension, pain, and movement restrictions.
IASTM (Instrument Assisted Soft Tissue Mobilization)
Instrument-assisted techniques to address soft tissue restrictions and pain.
Rehabilitation
A Typical Rehabilitation Progression
Three phases, from settling symptoms to returning to full activity.
Recovery from Carpal Tunnel Syndrome is usually staged: calm the symptoms first, then rebuild the strength and capacity of the area, then return to your full activities. The three phases below show the kind of progression the evidence supports and that I commonly work through in clinic. They are here to show you what the road can look like, not to act as a personal program.
- Phase 1
Pressure Reduction and Nerve Calm-Down (Weeks 1 to 4)
The priority in early management is lowering intracarpal tunnel pressure, particularly at night. Shi, Huisstede, and the AAOS Clinical Practice Guideline all converge on night splinting, activity modification, and gentle nerve mobilisation as the foundation of conservative care for mild to moderate cases. Nothing in this phase should provoke sharp pain or numbness during the exercise.
Examples, not a prescription
- Neutral-position wrist splint worn every night, confirmed to hold the wrist in true neutral (not extension)
- sliders, keeping elbow bent, opening and closing the hand while the wrist moves through a small pain-free range, 10 slow repetitions 3 to 4 times daily
- Tendon gliding sequence (straight, hook, fist, tabletop, straight fist), 5 repetitions of each position 3 times daily
- Ergonomic setup review: keyboard and mouse at elbow height, wrists kept close to neutral, vertical mouse if tolerated, micro-breaks every 20 to 30 minutes
- Task audit of sustained gripping activities (vibrating tools, heavy pinching), reducing peak duration rather than eliminating the task entirely
Ready to progress when
Nocturnal awakenings reduced compared with baseline, daytime symptoms no longer constant, and tolerated without provoking sharp symptoms for at least one to two weeks of consistent splint use.
- Phase 2
Restore Capacity in the Forearm and Wrist (Weeks 4 to 10)
Once the nerve is less irritable, start rebuilding the muscular support around the wrist, hand, and proximal chain. This phase is about increasing the hand's tolerance for daily loads without repeating the postures that compress the nerve. Proximal posture and scapular control matter here, because forward head and rounded shoulder postures increase neural tension the whole length of the median nerve.
Examples, not a prescription
- Thumb and opposition strengthening with a light band, 3 sets of 10 to 15, to maintain function
- Wrist flexor and extensor strengthening with a light dumbbell at slow tempo, 3 sets of 10 to 15, through a comfortable pain-free range
- Grip work with a soft ball or putty at submaximal effort, 3 sets of 10, progressing resistance as tolerance allows
- Scapular setting, rows, and external rotation with a light band, 3 sets of 10 to 12, to reduce proximal neural tension
- Progressive median nerve tensioners introduced at low dosage, only if sliders have been fully comfortable for 2 weeks
Ready to progress when
Nocturnal symptoms largely controlled with splint, no constant daytime numbness, grip strength improving on serial testing, and Boston Questionnaire scores trending downward by at least 1 point on symptom severity.
- Phase 3
Return to Work and Sustained Function (Weeks 10+)
Consolidate the gains and test whether the hand tolerates realistic workload without symptoms reappearing. The goal is to wean from the night splint, maintain the ergonomic and loading changes, and accept that for many people with a history of carpal tunnel syndrome, ongoing maintenance beats reactive flare management. If symptoms return during this phase despite compliance, surgical consultation moves up the priority list.
Examples, not a prescription
- Task-specific loading that mirrors real work demands (extended typing blocks, tool use intervals, sport-specific grip work) with scheduled micro-breaks
- Full-range wrist flexion and extension strengthening with moderate resistance, 3 sets of 8 to 12, 2 to 3 times per week
- Loaded carries such as farmer walks with moderate dumbbells, building grip endurance
- Periodic reassessment of sleep posture and nightly splint use, considering gradual weaning if symptoms remain absent
- Ongoing maintenance of scapular, , and mobility, particularly for desk workers
Ready to progress when
Night symptoms no longer requiring splint for control, daytime symptoms minimal or absent during full work duties, BCTQ symptom score within the normal range, and two consecutive weeks of unrestricted activity without a return of constant numbness.
Management
Prognosis & Recovery
What outcomes and recovery factors typically look like.
Expected timeline
Mild CTS: 60-70% improve within 4-8 weeks with night splinting and activity modification. Moderate CTS: 50-60% improve within 8-12 weeks with multimodal conservative care; those not improving require injection or surgical consultation. Severe CTS with constant numbness or : surgical decompression typically required, with 70-90% good outcomes but may have persistent mild symptoms if nerve damage was advanced
Natural history
Without treatment, symptoms typically progress from intermittent to constant over months to years. Approximately 30% spontaneously improve (especially pregnancy-related), 30% remain stable, and 40% progressively worsen with risk of permanent nerve damage including persistent numbness and permanent muscle weakness. Severe untreated CTS results in permanent sensory loss and irreversible motor deficit
Factors affecting recovery
Management
Measuring Progress
How to track the recovery arc week to week.
Day-to-day tracking
I track nocturnal symptoms (frequency of night waking, need to shake hands), daytime symptom patterns (constant vs intermittent numbness), functional limitations (buttoning, picking up small objects, grip tasks), and sensory testing of distribution. Measuring two-point discrimination and comparing to unaffected hand provides objective sensory measure. Grip strength dynamometry and pinch strength assessment track motor function
Assessment tools
Boston Carpal Tunnel Questionnaire (BCTQ) is the validated condition-specific outcome measure with symptom severity scale (11 items) and functional status scale (8 items). Minimum clinically important difference is 1.0 point reduction on symptom scale and 0.7 on functional scale. Levine-Katz questionnaire also widely used
Activity targets
Elimination of nocturnal symptoms requiring night waking, return to work tasks without symptoms (computer work, manual tasks), resumption of recreational activities requiring hand use (sports, musical instruments, crafts), and sustained improvement allowing weaning from night splint without recurrence
Management
Frequently Asked Questions
Common concerns and answers about this condition.
Why does my hand go numb at night with carpal tunnel syndrome?
Why does my hand go numb at night with carpal tunnel syndrome?
Most people sleep with their wrists curled into flexion, which dramatically increases pressure inside the . Sustained over several hours, that pressure starves the of oxygen, and you wake up with numbness, tingling, or aching that clears when you shake the hand out. This is the single most recognisable pattern of carpal tunnel syndrome, and it is why a neutral-position night splint is such a useful first-line intervention.
Do wrist splints actually help carpal tunnel syndrome?
Do wrist splints actually help carpal tunnel syndrome?
Yes, particularly at night and particularly in mild to moderate cases. The AAOS Clinical Practice Guideline on Management of Syndrome supports splinting as a non-operative option. Cochrane work by Page and colleagues (2012) on splinting also supported symptom relief compared to no treatment. Neutral position matters, because extension splinting also raises tunnel pressure. Compliance is the main factor I see separating people who get better from people who do not.
Do I need surgery for carpal tunnel syndrome?
Do I need surgery for carpal tunnel syndrome?
Not everyone. Mild to moderate cases respond to conservative care, including night splinting, activity modification, , and ergonomic changes. Shi and colleagues' 2020 systematic review comparing surgical and non-surgical treatment found surgery tends to produce larger long-term gains for patients who have more severe or persistent disease. I typically recommend surgical consultation when there is constant numbness, visible wasting, motor weakness, or when 6 to 12 weeks of appropriate conservative care has not changed the picture.
How long should I try splints and therapy before considering surgery?
How long should I try splints and therapy before considering surgery?
For mild to moderate cases, a fair trial is 6 to 12 weeks of consistent nightly splinting plus activity modification and . If you see clear symptom improvement in that window, I continue and re-evaluate at 12 weeks. If there is no meaningful change, or symptoms are progressing, I involve a surgical consult earlier rather than later. Severe cases with constant numbness or should proceed to surgical review straight away, because the nerve damage in that situation is not reliably reversible.
Can carpal tunnel syndrome go away on its own?
Can carpal tunnel syndrome go away on its own?
Sometimes. Pregnancy-related syndrome very often resolves within weeks of delivery as fluid shifts settle. Mild, activity-related cases can improve with load reduction alone. Most moderate or progressive cases, though, do not spontaneously resolve. They either plateau or worsen, which is why active management matters early rather than waiting to see.
Will nerve gliding exercises help?
Will nerve gliding exercises help?
Nerve and tendon gliding is a reasonable adjunct, and systematic reviews show mixed but generally positive results, particularly for mild to moderate cases when combined with splinting and activity change. They should feel comfortable, not sharp. If gliding exercises make symptoms worse, they are being done too aggressively or the nerve is more irritable than the current dosage tolerates.
Is carpal tunnel syndrome caused by typing?
Is carpal tunnel syndrome caused by typing?
Typing alone is not the whole story. The evidence for pure keyboard use as a direct cause is weaker than people assume. What I see more often is a combination of sustained wrist posture, repetitive forceful gripping, and underlying factors like pregnancy, diabetes, thyroid issues, higher body mass, or anatomically smaller tunnels. Changing the workstation helps many people, but if symptoms do not shift, I screen for the systemic contributors.
Why are my symptoms in both hands?
Why are my symptoms in both hands?
Bilateral syndrome is common, and often points to a systemic contribution rather than a purely mechanical one. Pregnancy, diabetes, hypothyroidism, and inflammatory all raise carpal tunnel pressure or compromise nerve resilience on both sides. When I see bilateral presentations, I check medical history more carefully and think about referring back to the family doctor for bloodwork if those have not been reviewed recently.
Related Conditions
Conditions I commonly see alongside, or confused with, this one.
- Common co-occurrence
Repetitive Strain Injuries
Carpal tunnel syndrome is a type of repetitive strain injury
- Anatomically related
De Quervain's Tenosynovitis
Both affect the wrist; can coexist due to similar risk factors
- Biomechanically linked
Tennis Elbow
Both can result from poor ergonomics and repetitive wrist/forearm motions