De Quervain's Tenosynovitis
Thumb tendon inflammation, common in new parents
Overview
The Science of De Quervain's Tenosynovitis
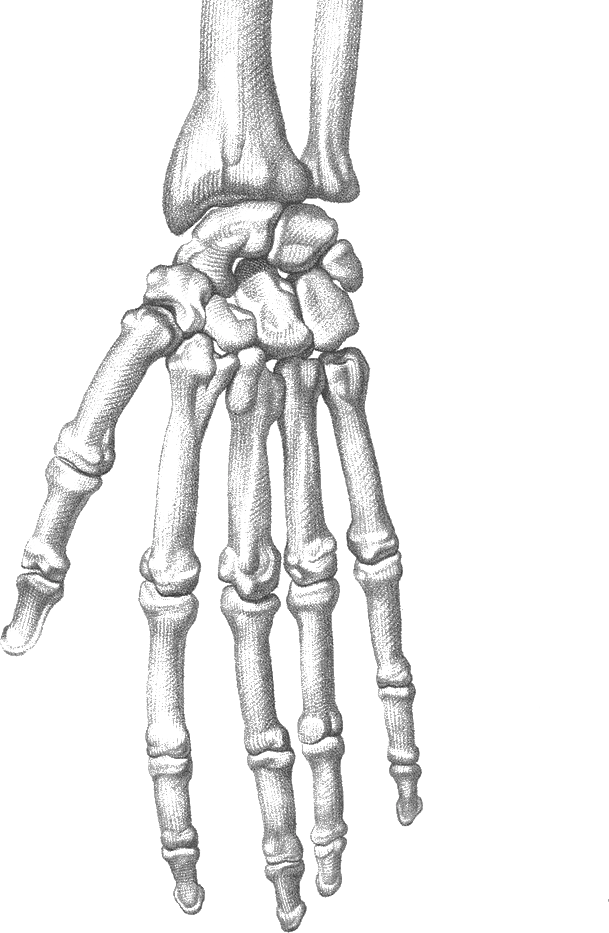
Link copiedDe Quervain's is a stenosing tenosynovitis affecting the first dorsal compartment of the wrist, specifically involving the pollicis longus (APL) and extensor pollicis brevis (EPB) tendons. These tendons pass through a fibro-osseous tunnel bordered by the radial styloid process and overlying extensor . The condition represents inflammation and thickening of the tendon sheath (tenosynovium) that creates a progressive (narrowing) of the compartment, mechanically restricting tendon glide and causing friction-induced inflammation.
The pathophysiological cascade begins with repetitive mechanical irritation from thumb movements combined with wrist deviation. This creates microtrauma to the tendon sheath lining, triggering an inflammatory response with synovial thickening, edema, and fibrous tissue deposition. As the sheath thickens, the space available for tendon excursion diminishes, creating a vicious cycle where normal movements cause progressively more friction and inflammation. Histologically, the sheath shows chronic inflammatory changes, metaplasia, and myxoid rather than acute inflammation, explaining why anti-inflammatory medications have limited efficacy.
Anatomical variations significantly influence susceptibility. Studies show 20-30% of individuals have multiple APL tendon slips (up to 4-5 separate slips), and approximately 50% have septations subdividing the first compartment into separate subcompartments for APL and EPB. These septations create additional friction points and explain why some cases respond poorly to injection therapy - the medication doesn't reach all affected compartments. The EPB may also have its own separate compartment in 10-20% of people, creating a variant anatomy that requires modified treatment approaches.
The condition shows strong demographic patterns: women are affected 6-10 times more frequently than men, with peak incidence in the 4th-6th decades. Pregnancy and early postpartum period represent particularly high-risk times due to hormonal influences on tendon and ligament combined with new repetitive infant care activities. Estrogen and relaxin affect metabolism and tendon material properties, potentially predisposing to inflammatory conditions. Risk factors include diabetes mellitus (2-3 times higher prevalence), rheumatoid , hypothyroidism, and previous wrist trauma or fracture.
The condition frequently coexists with other thumb including carpometacarpal (CMC) arthritis, intersection syndrome (inflammation where APL/EPB cross over wrist extensors), and syndrome. Differential diagnosis requires careful assessment as these conditions can produce overlapping symptoms but require different management approaches.
Overview
Contributing Factors
Link copiedThe biomechanical drivers of De Quervain's center on repetitive thumb movements combined with ulnar deviation of the wrist - a movement pattern that maximally tensions and deviates the APL and EPB tendons through the first dorsal compartment. The classic provocative movement involves lifting or grasping with the thumb abducted while simultaneously bending the wrist toward the ulnar side (little finger direction). This combination creates maximum angulation and friction as the tendons change direction around the radial styloid process.
The "new mother" presentation is the archetypal example of biomechanical overload. Repeatedly lifting an infant requires sustained thumb and extension to support the baby's head and neck, combined with wrist ulnar deviation and slight flexion - the exact position that maximally loads the first compartment tendons. The "baby lift" movement performed dozens of times daily, often while sleep-deprived and with altered posture from breastfeeding, creates cumulative microtrauma exceeding tissue repair capacity. Studies show new mothers have 4-5 times higher incidence compared to age-matched nulliparous women, with symptoms typically appearing 4-12 weeks postpartum when infant lifting demands peak.
Smartphone and texting activities contribute significantly to modern De Quervain's incidence. Thumb-intensive texting maintains the thumb in repetitive abduction and extension against resistance, while the wrist often adopts ulnar deviation to balance the device weight. Gaming with controllers requiring sustained thumb movements shows similar biomechanical loading. The sustained nature of these activities prevents adequate recovery periods between loading cycles, promoting chronic inflammation. Research shows smartphone users averaging over 6 hours daily have 3 times higher incidence compared to minimal users.
Occupational activities create high-risk scenarios. Hairdressing requires sustained pinch grip with scissors while the wrist deviates to angle the cut - thousands of repetitions daily with the thumb in sustained abduction against resistance. Gardening, particularly pruning with secateurs or hand shears, combines forceful pinch grip with wrist deviation. Assembly work requiring repeated thumb-operated tools (staplers, precision screwdrivers, tweezers) maintains continuous loading without relaxation. Even office work involving extended mouse use can contribute if the thumb maintains sustained extension to control buttons while the wrist adopts awkward postures.
Daily activities that seem innocuous create cumulative loading. Wringing towels or washcloths requires forceful pinch grip combined with repetitive twisting - the wrist moves into ulnar deviation as you wring, while the thumb works hard to maintain grip. Opening jar lids combines thumb abduction force with wrist torque. Lifting pots, pans, or kettles by their handles with thumb-up grip position loads the tendons maximally. Knitting and crochet maintain sustained thumb positioning with repetitive fine motor control requiring continuous APL/EPB activation.
The anatomical path of these tendons creates inherent vulnerability. As they travel from the forearm to the thumb, they must navigate a sharp angle around the radial styloid - essentially making a 45-60 degree turn through a narrow tunnel. Any movement combining thumb abduction with wrist ulnar deviation tightens this angle further, compressing the tendons against the radial styloid like a rope pulled taut around a pulley. The more acute the angle, the higher the friction and pressure within the compartment.
Grip technique and tool design dramatically influence loading. Larger diameter handles requiring wider thumb-finger spread increase APL/EPB activation compared to smaller diameter grips. Tools positioned to maintain neutral wrist position reduce tendon deviation through the first compartment compared to designs forcing wrist deviation. Power grip patterns (full hand around object) distribute forces across multiple tendons, while pinch grip patterns (thumb opposing fingers) isolate loading to thumb tendons including APL/EPB. Poor proximal stability forces compensatory thumb overuse - weak shoulder and scapular stabilizers cause people to generate precision movements with distal muscles (thumb and wrist) rather than controlling from proximal structures.
Symptoms
Clinical Presentation
Link copiedPrimary Symptoms
Associated Symptoms
Typical pattern
Gradual onset over weeks to months, often associated with new repetitive activity (infant care, gardening, increased texting/gaming). Pain initially present only with specific movements, progressively becomes more constant and present with simple activities. Often bilateral but may be asymmetric. Strong female predominance, particularly postpartum women or those in 40-60 age range.
Symptoms
Differential Diagnosis
Link copiedConditions with similar presentations:
Carpometacarpal (CMC) Arthritis (Thumb Base Arthritis)
Key differences: Pain localized to thumb base joint (more distal than De Quervain's), worse with pinch and grip loading, positive grind test (axial compression and rotation of thumb), visible prominence or squaring of thumb base, X-ray shows joint space narrowing and
Intersection Syndrome
Key differences: Pain 4-6 cm proximal to radial styloid where APL/EPB cross over wrist extensors, may have visible swelling and , positive with resisted wrist extension and radial deviation, more proximal than De Quervain's
Scaphoid Fracture (Acute or Non-union)
Key differences: History of fall on outstretched hand, pain in anatomical snuffbox, pain with axial loading of thumb, positive scaphoid compression test, requires imaging
Superficial Radial Nerve Neuritis (Wartenberg's Syndrome)
Key differences: Burning, tingling pain over dorsoradial wrist and hand, positive Tinel's sign over superficial radial nerve, symptoms with wrist flexion and ulnar deviation (opposite of De Quervain's), no 's pain
Scapholunate Ligament Injury
Key differences: Pain more central in wrist, painful click with radial-ulnar deviation, positive Watson's test (scaphoid shift), weakness with grip, history of wrist trauma
When to seek professional help
Research
Key Research & Evidence
Peer-reviewed studies supporting the treatment approach.
Finding
Ultrasound-guided corticosteroid injection is more accurate than blind injection, and anatomical septations are common in De Quervain's disease
Research details
A systematic review and meta-analysis by Abi-Rafeh and colleagues (Plastic and Reconstructive Surgery, 2022) examined ultrasound use in De Quervain's disease. It found that an intercompartmental septum was significantly more common in the surgical De Quervain's population than in the general cadaveric population (67% versus 35%). Ultrasound-guided corticosteroid injections were more accurate than manual landmark-based injections (90 to 100% versus 40 to 100% accurate placement) and were associated with better reported treatment success rates (73 to 100% versus 59 to 83%)
Clinical relevance
Anatomical variations including compartment septations are common and significantly impact injection success. Ultrasound guidance substantially improves outcomes by ensuring accurate placement and complete compartment coverage. When injection is indicated, ultrasound guidance should be used when available to maximize success and minimize need for repeat injections or surgery
Finding
Combining a thumb orthosis with corticosteroid injection is more effective than either treatment alone for De Quervain's disease
Research details
A systematic review and meta-analysis by Cavaleri and colleagues (Journal of Hand Therapy, 2016) compared corticosteroid injection with hand therapy in De Quervain's disease. Both injection and hand therapy improved pain and function from baseline, with no significant difference between the two approaches across the trials examined. However, significantly more people were treated successfully when a combined orthosis plus corticosteroid injection approach was used than with an orthosis alone (relative risk 0.53, 95% CI 0.35-0.80) or injection alone (relative risk 0.76, 95% CI 0.64-0.89), supporting a combined conservative approach
Clinical relevance
Splint design and duration significantly impact outcomes. Optimal results require comprehensive thumb and wrist immobilization for minimum 4 weeks combined with activity modification - shorter durations or less restrictive splints produce inferior results. Patient education regarding compliance critical as many discontinue splinting prematurely when initial symptoms improve, leading to recurrence
Finding
Pregnancy and the postpartum period are recognised high-risk times for De Quervain's tenosynovitis, with specific gestational risk factors identified
Research details
A population-based study by Bae and colleagues (Clinics in Orthopaedic Surgery, 2022) using South Korean national insurance data found pregnancy-related De Quervain's tenosynovitis in roughly 2.1 of every 100 pregnant women (34,342 cases among 1,601,501 pregnancies), with age 30 years or older, multiple gestation, cesarean delivery, hypertensive disorders of pregnancy, and underlying rheumatoid arthritis identified as significant risk factors. A separate case-control study by Daglan and colleagues (Hand (N Y), 2023) of 63 postpartum women with De Quervain's compared with 630 controls found that a pregnancy longer than 40 weeks (odds ratio 5.81) and first childbirth (odds ratio 2.23) were associated with higher risk
Clinical relevance
Pregnancy and early postpartum represent extremely high-risk period due to combined hormonal and biomechanical factors. However, high spontaneous resolution rate by 6 months postpartum as hormones normalize and infant lifting technique improves supports conservative management as first-line approach. Early intervention with splinting and ergonomic education for infant care can prevent progression to chronic cases. Patients should be counseled that conservative treatment success rate is higher than in non-pregnancy-related cases
Management
Evidence-Based Management
Treatment strategies with the strongest support in the current literature.
Primary approach
Thumb spica splinting immobilizing the thumb and wrist combined with activity modification achieves symptom resolution in 70-80% of cases within 4-6 weeks by reducing friction within the first dorsal compartment and allowing inflammatory resolution
Complementary
Corticosteroid injection into the first dorsal compartment provides 60-80% success rate when splinting fails, with higher efficacy when ultrasound-guided to ensure medication reaches all compartment septations. and tendon gliding exercises address mobility restrictions and prevent adhesions
Prevention & long-term
Modified lifting technique (supporting baby's weight on forearm rather than with extended thumb), ergonomic tool and smartphone use, and thumb and wrist strengthening lower the risk of recurrence in high-risk groups including new mothers and repetitive workers
Detailed management strategies
Thumb Spica Splinting Protocol
Immobilizes thumb interphalangeal joint and wrist in neutral position, preventing the thumb and wrist deviation that creates friction within the first dorsal compartment. Reduces inflammation by minimizing repetitive mechanical irritation. Off-the-shelf or custom splints should extend from mid-forearm to thumb tip, leaving thumb tip free for sensation
Important precautions
- Wear continuously for first 2-3 weeks, then during high-demand activities for additional 3-4 weeks
- Remove only for hygiene and prescribed exercises
- Ensure splint maintains wrist in neutral (not extension which increases compartment pressure)
- Monitor for skin irritation, numbness, or excessive swelling indicating too-tight application
Activity Modification for Infant Care (New Mothers)
Modifying infant lifting technique from thumb-intensive to forearm-supported dramatically reduces tendon loading. Supporting baby's weight on forearm with palm up (supinated) rather than palm down with extended thumb distributes forces across larger muscles and avoids first compartment loading. Using both hands for all lifts further reduces load per side
Important precautions
- Support baby's head/neck on your forearm rather than with extended thumb
- Use palm-up carry position whenever possible
- Engage core and use legs for lifting rather than arms alone
- Alternate sides to prevent overload
- Use nursing pillows, baby carriers, and positioning aids to minimize repetitive lifting
Ergonomic Tool and Device Modifications
Modifying grip patterns and tool designs reduces cumulative thumb and wrist loading. Larger diameter handles distribute pressure across greater surface area. Neutral wrist positioning during activities minimizes tendon angulation through first compartment. Frequent position changes and microbreaks prevent sustained loading
Important precautions
- Use smartphone holders or voice-to-text rather than sustained thumb texting
- Hold phone with fingers supporting back, not thumb extending to reach screen
- Choose tools with padded, larger diameter handles
- Position work to maintain wrist in neutral (not deviated or extended)
- Take 30-second breaks every 10-15 minutes during repetitive activities
Tendon Gliding Exercises
Specific exercises that gently mobilize APL and EPB tendons through the first compartment, reducing adhesions and maintaining mobility during healing. Performed within pain tolerance to avoid aggravating inflammation. Maintain tendon excursion while minimizing friction by avoiding end-range provocative positions
Important precautions
- Begin only after initial acute inflammation controlled (typically 2-3 weeks)
- Perform slowly and gently - 5 repetitions, 3-5 times daily
- Should not cause sharp pain; mild discomfort acceptable
- Avoid Finkelstein position (fist with thumb tucked, wrist deviation) until late rehabilitation
Ice Application for Acute Flare-ups
Local cooling reduces inflammation, decreases pain perception through neural mechanisms, and minimizes secondary muscle guarding. Most effective when applied after activities or during acute symptom exacerbations
Important precautions
- Apply ice 15-20 minutes, 3-4 times daily during acute phases
- Use barrier (towel) between ice and skin to prevent ice burn
- Most effective when applied directly over radial styloid
- More helpful in first 2-4 weeks; less effective for chronic symptoms
Progressive Strengthening (Late Phase)
Once inflammatory symptoms controlled, systematic strengthening of thumb , extensors, and wrist stabilizers improves load tolerance and prevents recurrence. Strengthening proximal stability (shoulder, scapula) reduces compensatory distal overuse
Important precautions
- Begin only after wearing splint during day no longer needed (typically 6+ weeks)
- Progress from isometric to light resistance to functional strengthening
- Avoid return to high-repetition thumb-intensive activities until strength restored
- Address full kinetic chain including shoulder and scapular stability
Management
Treatment Techniques
Evidence-based manual therapy and intervention approaches.
Treatment approaches supported by current research and clinical guidelines
Recommended treatment approaches
Treatment approaches are individualized to each patient's needs and goals. All interventions require explicit informed consent, and treatment plans are collaboratively modified based on your preferences and response to care.
Dry Needling
Precise needle therapy targeting trigger points for effective pain relief and improved muscle function.
Soft Tissue & Myofascial Therapy
Targeted hands-on techniques to address muscle tension, pain, and movement restrictions.
IASTM (Instrument Assisted Soft Tissue Mobilization)
Instrument-assisted techniques to address soft tissue restrictions and pain.
Rehabilitation
A Typical Rehabilitation Progression
Three phases, from settling symptoms to returning to full activity.
Recovery from De Quervain's Tenosynovitis is usually staged: calm the symptoms first, then rebuild the strength and capacity of the area, then return to your full activities. The three phases below show the kind of progression the evidence supports and that I commonly work through in clinic. They are here to show you what the road can look like, not to act as a personal program.
- Phase 1
Calm the compartment (Weeks 1 to 3)
The first job is to reduce friction at the first dorsal compartment and take the sting out of daily tasks. That means consistent thumb spica use, pain-free movement only, and a deliberate audit of how the thumb is being loaded during the day. Nothing in this phase should reproduce the sharp radial-sided pain.
Examples, not a prescription
- Off-the-shelf or custom thumb spica that immobilises the wrist and the thumb IP joint, worn during waking hours for 2 to 3 weeks
- Pain-free thumb IP and MCP flexion and extension, 10 slow repetitions 3 times daily, to prevent stiffness
- Lifting technique coaching for new parents: wide forearm-supported scoop, palm-up where possible, thumbs tucked close to the hand
- Ice over the radial styloid 10 to 15 minutes after aggravating activities if it helps symptoms
- Task audit: reduce sustained pinching (phone scrolling, gardening shears, scissors) rather than eliminating every activity
Ready to progress when
Tenderness at the radial styloid clearly reduced, still uncomfortable but no longer sharp, and the thumb can move through pain-free range without a flare for one to two weeks of consistent splint use.
- Phase 2
Rebuild tolerance (Weeks 3 to 8)
Once the sheath is calmer, start restoring capacity in the thumb, wrist, and proximal chain. The aim is to tolerate everyday loads again without re-igniting the compartment. Proximal posture and scapular control matter, because distal overuse often reflects a poorly supported upper chain.
Examples, not a prescription
- thumb and extension holds, 5 seconds on, 5 seconds off, 3 sets of 10, at a load that never provokes radial-sided pain
- Tendon gliding through the first compartment: pain-free thumb circumduction and opposition, avoiding the Finkelstein end-range until symptoms are gone
- Wrist flexor and extensor strengthening with a light dumbbell, slow tempo, 3 sets of 10 to 15 through a comfortable range
- Scapular setting, rows, and external rotation with a light band, 3 sets of 10 to 12, to unload a poorly supported upper chain
- Weaning the splint during low-demand activities first, keeping it on for baby care, gardening, or sustained pinching
Ready to progress when
Finkelstein's test no longer sharp, tenderness at the radial styloid minimal to absent, thumb abduction strength symmetrical on manual testing, and everyday tasks like jar-opening or infant care tolerated without a flare.
- Phase 3
Return to real demand (Weeks 8+)
Now the hand has to tolerate the demands that caused the problem in the first place, often infant care, occupational pinching, or racquet and stick sports. The goal is full, resilient thumb and wrist loading, with technique changes kept in for the long run. If a flare happens here, the plan pulls back one phase rather than starting from scratch.
Examples, not a prescription
- Task-specific loading that mimics real demand: longer holds with infant care, sustained tool use, sport-specific grip work, with planned micro-breaks
- Full-range thumb and wrist strengthening with moderate resistance, 3 sets of 8 to 12, two to three times per week
- Grip and pinch progression with a dynamometer or putty, targeting symmetry with the uninjured side
- Loaded carries (farmer walks) with moderate dumbbells for grip endurance
- Ongoing and scapular maintenance work, particularly for desk workers and new parents who spend long hours feeding in supported positions
Ready to progress when
Two consecutive weeks of full daily and occupational demand without pain, symmetrical thumb and grip strength, no need for the splint outside of heavy one-off tasks, and a clear plan for what to do if a flare appears.
Management
Prognosis & Recovery
What outcomes and recovery factors typically look like.
Expected timeline
Mild cases: 60-70% achieve significant improvement within 4-6 weeks with thumb spica splinting and activity modification. Moderate cases: 70-80% improve within 8-12 weeks with comprehensive conservative care. Cases failing 6-8 weeks of appropriate conservative treatment: 60-80% respond to single corticosteroid injection. Surgical treatment (when needed): over 90% success rate with low recurrence
Natural history
Without treatment, symptoms typically persist with gradual worsening over months to years. Spontaneous resolution occurs in approximately 30-40% of mild cases, particularly postpartum cases once hormonal factors normalize and infant lifting demands decrease. However, 60-70% either persist or worsen without appropriate intervention. Chronic untreated cases develop progressively more sheath thickening and fibrosis, making eventual treatment more difficult and often requiring surgical release
Factors affecting recovery
Management
Measuring Progress
How to track the recovery arc week to week.
Day-to-day tracking
I track pain levels during specific activities (pinch grip, wrist deviation, lifting objects), tenderness on palpation over the first dorsal compartment using pressure algometry when available, grip and pinch strength measurements comparing to unaffected side, and functional limitations with daily tasks. Positive 's and Eichhoff's tests are repeated to assess provocative test response
Assessment tools
Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire is the validated outcome measure for upper extremity conditions. Patient-Rated Wrist Evaluation (PRWE) also used for wrist-specific assessment. Numeric Pain Rating Scale (0-10) tracked for pain at rest and with specific activities. Visual analog scale for subjective swelling sensation
Activity targets
Pain-free infant lifting and care for new mothers, return to occupational activities requiring repetitive thumb use (hairdressing, gardening, assembly work) without limitation, resumption of recreational activities (crafts, texting, gaming, sports) with proper technique, and sustained improvement allowing discontinuation of daytime splinting without recurrence
Management
Frequently Asked Questions
Common concerns and answers about this condition.
Why does my thumb-side wrist hurt so much when I lift my baby?
Why does my thumb-side wrist hurt so much when I lift my baby?
That specific pattern, sharp pain on the radial wrist just above the thumb when you scoop a baby up under the arms, is the textbook De Quervain's presentation. The scoop loads the pollicis longus and extensor pollicis brevis tendons as they bend around the radial styloid. New parents repeat that movement dozens of times a day, often with the wrist deviated and the thumb extended under load. It is one of the most common reasons post-partum patients end up in front of me.
Is Finkelstein's test enough to diagnose this?
Is Finkelstein's test enough to diagnose this?
It is the cornerstone of the clinical diagnosis, but it is not the whole picture. A positive 's combined with tenderness directly over the first dorsal compartment and a story that fits (new parenting, a spike in thumb-loading activity, hairdressing, racquet sports) is usually all you need. What I am also doing is ruling out thumb CMC , intersection syndrome, a scaphoid problem, and superficial radial nerve irritation. Those can all sit close by and be mistaken for each other.
Do I really have to wear a thumb spica splint?
Do I really have to wear a thumb spica splint?
Yes, and consistency matters. A thumb spica that holds the wrist and the thumb interphalangeal joint still takes load off the first compartment and lets the sheath calm down. Huisstede and colleagues' 2018 systematic review in Archives of Physical Medicine and Rehabilitation supports splinting, particularly combined with corticosteroid injection when injection is needed. Two or three weeks of consistent use usually makes a noticeable difference. Wearing the splint only when convenient is the most common reason I see treatment stall.
Will a cortisone injection fix this?
Will a cortisone injection fix this?
For many people with a confirmed De Quervain's, a well-placed corticosteroid injection into the first dorsal compartment helps significantly, particularly when combined with a thumb spica. Anatomical septations are common, and injections that miss a septated sub-compartment do not work as well, which is why ultrasound-guided injection tends to outperform landmark-based in the literature. Injection is not something I do myself, but I often coordinate with the physician who does.
How long until it settles?
How long until it settles?
Most mild and moderate cases I see meaningfully improve within four to six weeks of consistent splinting, activity modification, and graded exercise. Post-partum cases often continue to settle over a few months as the hormonal picture shifts and the lifting pattern improves. Cases that have been smouldering for more than six months, or that have already failed injection, tend to be slower and sometimes end up at a surgical consult.
Can I still pick up my baby?
Can I still pick up my baby?
Yes, but the technique needs to change. Scooping under the arms with the thumb sticking out is the exact movement that keeps irritating the tendons. I coach patients to scoop with a wider, forearm-supported lift, palm-up where possible, keeping the thumbs close to the side of the hand rather than flared out. Small changes to how you lift, burp, and feed add up quickly over a day.
Do I need surgery?
Do I need surgery?
Usually not. Surgical release of the first dorsal compartment is effective when it is needed, but the path almost always starts with a thumb spica, activity change, and graded rehab, then a corticosteroid injection if conservative care plateaus. Surgery is reserved for people who have failed a proper trial of conservative care including injection, or for clear anatomical reasons like a separate EPB sub-compartment that keeps blocking injection success.
Related Conditions
Conditions I commonly see alongside, or confused with, this one.
- Common co-occurrence
Repetitive Strain Injuries
De Quervains is a repetitive strain injury affecting thumb tendons
- Anatomically related
Carpal Tunnel Syndrome
Both affect wrist structures; similar risk factors and can coexist
- Anatomically related
Wrist Sprains & Strains
Both affect wrist region; acute injuries can predispose to De Quervains
Get Expert Treatment
Professional physiotherapy for de quervain's tenosynovitis